


Κωνσταντίνος
Ορθοπαιδικός
Bougoulias.com | © 2022 | All rights reserved
Μπουγουλιάς
Χειρουργός





The latest HTML5, CSS3 and advanced JavaScript have
been used to ensure the highest compatibility.






Δημοσίευση περιστατικού οστεοχονδρώματος
μηρού αντιμετωπισθέν στο Αφγανιστάν.
Patient:
Age: 14 years
Sex: male
Clinical summary:
Palpable mass in the right knee.
Clinical history and imaging procedures:
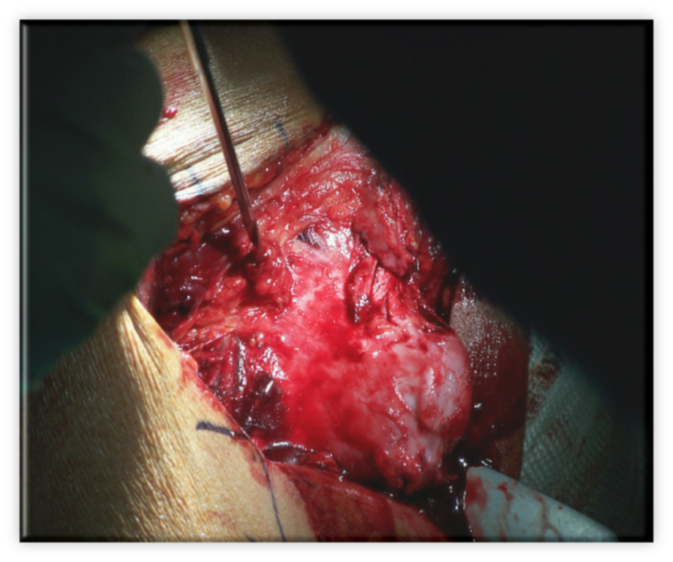
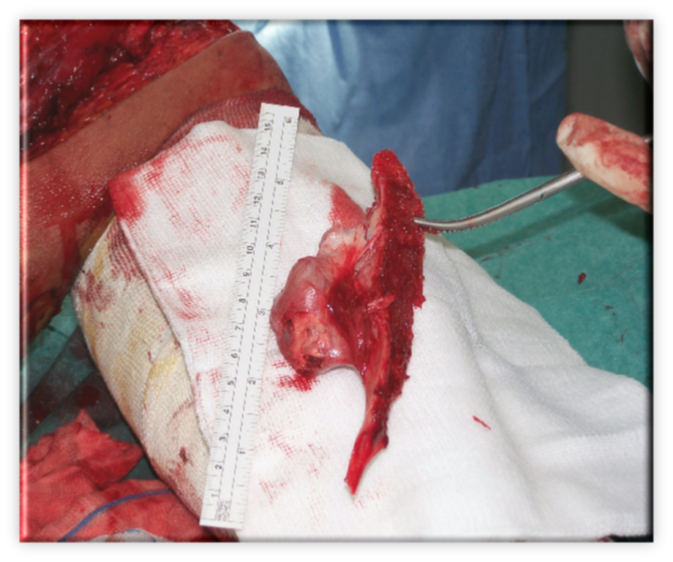
The patient referred to our field military hospital in Kabul, Afghanistan, complaining for a palpable mass over the right distal femur which was first noticed two years ago. The mass change in size within the last year (got bigger) and the patient was filling a mild tense on his skin. An AP and a lateral radiograph of the knee were performed revealing a tumour 8 x 3.8cm in the medial posterior aspect of the distal femur. The tumour was pedunculated, cauliflower in shape, with the pedicle merging smoothly with the normal cortex of the bone. In the distal portion of the lesion the characteristic chondroid calcification is observed. The findings were diagnostic for osteochondroma of distal femur. The patient tolerated well the surgical removal of the tumour and the diagnosis was confirmed by the pathologist.
Discussion:
Osteochondroma (osteocartilaginous exostosis) is the most common tumour of bone and represents approximately 40% to 44% of benign bone lesions. It is a neoplasm composed of a cartilaginous bony projection arising from the surface of bones. Most patients with osteochondroma are under 20 years of age. Grossly, osteochondromas can be of two types, sessile or pedunculated. The most common locations are the metaphysis of the distal end of the femur, the proximal end of the tibia, and the humerus. Other sites are the proximal femur, scapula, fibula, ilium, and distal tibia. Rarely an exostosis arises in the spine.
Osteochondromas can be manifested clinically in several ways. A mass may be noted on palpation of the affected limb or found accidentally during a radiographic examination. Pain may be the presenting symptom. It is often secondary to pressure on adjacent soft tissues, vessels, and nerves, or it may be the result of a pathologic fracture. Rarely, a bursa develops over the osteochondroma (bursa exostotica), and the patient may experience acute pain and swelling. Fewer than 2% of exostoses will continue to grow after closure of the adjacent growth plate (skeletal maturity).
The radiographic features are characteristic and are almost enough for the diagnosis. An osteochondroma arises from the metaphyseal-


1a. A tumour over the medial posterior aspect of the distal femur pedunculated, cauliflower in shape, with the pedicle merging smoothly with the normal cortex of the bone. Note the characteristic chondroid calcification.

1b. Osteoblastoma over the distal femur pointing characteristically away from the joint.
[1] Miller M. Review of Orthopaedics. Saunders, Philadelphia, pp464-
[2] Karasick D, Schweitzer ME, Eschelman DJ. Symptomatic Osteochondromas: Imaging Features. AJR 1997 June; 168(6):507-
[3] Resnick D. Diagnostic of bone and joint diseases. WB Saunders, Philadelphia, pp 3725-
2a. Postoperative lateral radiograph of the right knee
μηρος, μηρός, οστεοχονδρωμα μηρου, οστεοχόνδρωμα μηρού
